

The Root Causes of Gender Dysphoria
From social influence to bacteria, viruses, and chemicals - and what you can do to resolve distressing symptoms impacting you or your children

Disclaimer: This article explores possible root causes of transgender identity and gender dysphoria, including biological, environmental, and social factors such as microbes, chemicals, and cultural influences. It also discusses non-medical perspectives and potential interventions outside the mainstream use of hormones and surgeries, which are quite controversial and potentially harmful to many.
This exploration is driven by open inquiry, not by bias. Investigating the underlying factors of any human experience, no matter how sensitive or politically charged, is not inherently an act of prejudice. The intention here is to consider a wide range of contributing factors with curiosity and care.
In plain terms: this article is not transphobic. It does not express hate or judgment, but rather seeks to understand complex experiences more deeply.
Definitions
The transgender identity and experience of gender dysphoria has become one of the most controversial topics in our society.
Currently, these are seen as two different but potentially overlapping issues with the following definitions:
Transgender - A person whose gender identity does not correspond with the sex registered for them at birth
Gender dysphoria - A sense of unease due to incongruence between ones experienced gender and the one registered for them at birth
You will notice that these definitions are very similar. The key difference is that gender dysphoria involves a sense of unease, and it is currently thought that not everyone who is transgender experiences unease.
The mainstream school of thought is that being transgender is an identity whereas having gender dysphoria is a medical condition (identified in the DSM-5) that not all transgender people experience.
However, I’m not entirely sure that the differentiation in these definitions is accurate. I think incongruity between ones perceived gender and the sex they were born with entails an inherent unease. And, I think these definitions have little to do with the people they describe and everything to do with the medical model of how we treat these identities and conditions.
Mainstream Treatment
While being transgender is not considered a medical diagnosis, it does have an identified set of medical treatments. It has the same identified set of medical treatments, in fact, as gender dysphoria. Which begs the question - if it has identified medical treatments, is it not a diagnosable medical condition?
The current Standard of Care - that is, the acceptable medical treatment for any given condition - for both being transgender and experiencing gender dysphoria is “gender affirming care.” Which means confirming that the persons identity is in fact incongruent with their physical body, and includes a plethora of medications and surgeries. They’re the same exact treatments, including but not limited to:
Puberty blockers in children to delay the natural onset of puberty
Hormone therapy including estrogen and anti-androgens, and testosterone
Gender affirming surgery including:
mastectomies (breast removal) and breast augmentation (implants) also referred to as “top surgery;”
vaginoplasty, vulvoplasty, phalloplasty, metoidioplasty, hysterectomy, oophorectomy, and orchiectomy also referred to as “bottom surgery;”
and other plastic surgeries including facial feminization or masculinization, tracheal shave (Adam’s apple reduction), voice surgery, and other body contouring (liposuction, fat grafting, other implants like butt and hip, etc)
While these surgeries are largely cosmetic, they are not considered cosmetic surgeries - they are considered medically necessary in order to reduce dysphoria.
However, unfortunately, there are many studies with large datasets showing that these surgeries may actually not reduce dysphoria and distress as the odds of suicide in transgender individuals actually increases after gender-affirming surgery.
These treatments and surgeries also significantly interfere with or completely inhibit reproduction, and are often undertaken in those who are at an age that their frontal lobe hasn’t fully developed (which happens in the mid-20s to early 30s), meaning they may not fully understand the consequences of their decisions.
Effectiveness and Profitability
So why is the Standard of Care increasing suicidality in this population?
Well, one reason is that the Standard of Care has been conflated with a moral imperative to believe people’s perceptions of themselves are 100% accurate - even though that’s not how we treat other issues of body image and distress, like body dysmorphia which is often associated with disordered eating.
We would never affirm that someone with an eating disorder’s incorrect view of themselves as fat was actually correct, nor would we offer them cosmetic surgeries and liposuction to match their body to their delusion. We would, rightfully, pathologize that as severe mental illness.
Another reason the Standard of Care is upheld despite the evidence that it exacerbates distress is that it is incredibly profitable.
When you consider that approximately 75% of individuals with gender dysphoria report experiencing it initially in early childhood, and that medical transition often involves a lifetime of hormones and multiple surgeries, it's no surprise that the estimated profit generated from a single transitioning patient can exceed $1 million - making it one of the most lucrative pathways in modern medicine.
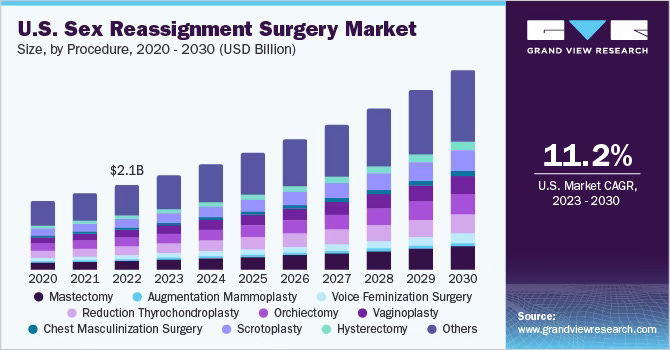
Additionally, the total U.S. sex reassignment surgery market size was estimated at $2.1 billion in 2022 and is anticipated to grow at a compound annual growth rate of over 11% annually - reaching $5 billion by 2030.
Root Causes of Gender Dysphoria
So if the Standard of Care is built on false premises - what if there are other treatment options that would be more effective at reducing distress in this population?
What if there are scientific root causes of the transgender identity that could be addressed to reduce the dysphoria, without permanent medical interventions to alter one’s apparent sex?
First, it is important to understand what the current theory is with regard to where and how gender dysphoria and the transgender identity arise from.
Many scientists currently believe that gender dysphoria arises from incorrect “brain sex” - meaning this theory surmises that because the brains of people with gender dysphoria look more like the opposite sex than the one they are born with, there is an actual mismatch between one’s sex at birth and one’s identity.
However, a 2019 study by neurologist Stephen Gliske put forth a Multisense Theory of Gender Dysphoria, challenging the current assumptions around why the brain may develop in this way.
Multisense Theory of Gender Dysphoria
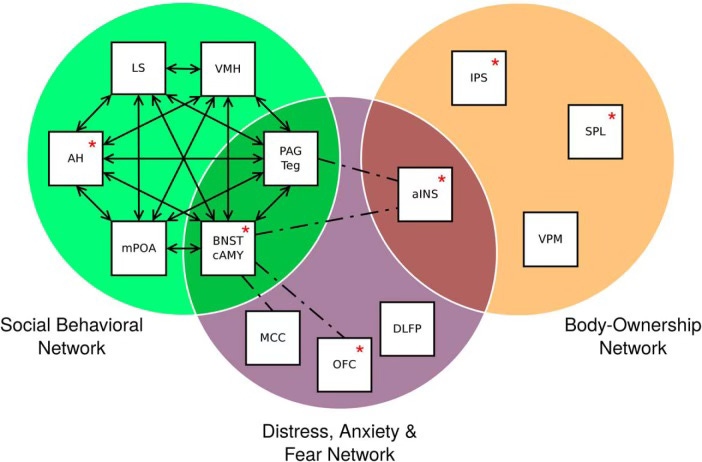
Using a meta-analysis of available brain data, this study identified that gender dysphoria arises through structural brain differences that exist in three interrelated brain networks:
Distress, Anxiety and Fear Network - related to emotional pain and discomfort
Social Behavioral Network – connected to interactions and identity
Body Ownership and Perception Network – how we perceive our body as our own
If activity in these networks is altered or disconnected, the theory proposes that could contribute to the distress felt in gender dysphoria. Preexisting brain imaging studies have hinted that changes in these networks, rather than just physical brain structure, may be linked to the experience of gender dysphoria.
The specific brain networks involved are shown and described in Figure 2 and its caption below.
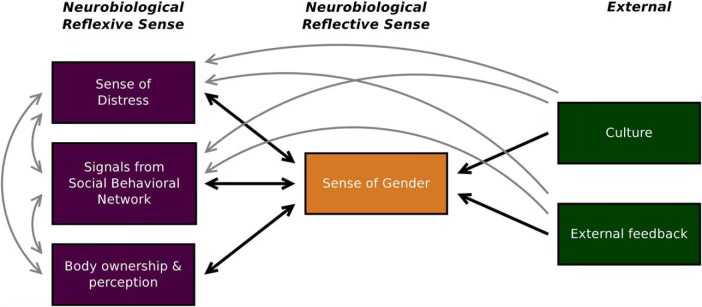
The Multisense Theory of Gender Dysphoria also models that senses based on these networks are integrated with each other and other factors - including external cultural and social feedback - resulting in an overall sense of gender, as shown below. The underlying neurobiology would influence how much an individual feels chronic distress, how much they desire to act in a manner consistent with their gender role, and how much they feel the gendered aspects of their body belong to them - all of which then contributes to the extent to which an individual feels that their gender matches that which was assigned at birth (i.e. their overall sense of gender).
Unfortunately - because this theory upends the currently accepted theory of gender dysphoria, and has implications for treatment recommendations, despite being double-blind peer reviewed and scientifically sound - this article was retracted under immense social pressure in mid-2020.
Initially, the journal who originally published the study pressured Gliske to remove the clinical recommendations at the end of the study, which he obliged. But critics of this study and its conclusions were not happy with that and launched a change.org petition to have it retracted altogether, stating that “the clear intent of the paper was to do harm to the transgender community.” They succeeded in getting the study retracted altogether. This is but one in a series of instances in which scientific study of transgender identity and gender dysphoria is challenged or silenced when it questions the current (profitable) status quo.
Causes of Gender Dysphoria
Looking at this issue through the lens of the Multisense Theory of Gender Dysphoria allows one to consider that there might be triggering events preceding the experience of gender dysphoria.
So what might those be? And when and how might they occur?
According to a 2020 study by Cedars-Sinai Medical Center titled “Age at First Experience of Gender Dysphoria Among Transgender Adults Seeking Gender-Affirming Surgery,” 73% of trans women and 78% of trans men first experienced gender dysphoria by age 7.
What happens at age 7?
An early stage of puberty called adrenarche begins. This is when the adrenal glands start producing a hormone called dehydroepiandrosterone (DHEA). DHEA is involved in the development of pubic hair, oily skin, oily hair, and body odor as well as sexual attraction/sexual desire/increased libido.
Adrenarche, a developmental phase leading up to puberty and occurring between ages 6 and 9, is when a person first develops hormones that directs them towards sexual attraction to others, which can, in turn, affect their own sexual and gender identity.
Critically, the adrenal glands comprise part of the the hypothalamic–pituitary–adrenal (HPA) axis related to acute stress, which is a key part of the BNST in the brain - which is involved in the Distress, Anxiety, and Fear Network and the Social Behavioral Network identified in the Multisense Theory of Gender Dysphoria. In those who identify as transgender or experience gender dysphoria, the BNST notably is closer in size to that of the opposite sex.
Comorbid Conditions
Comorbid conditions of gender dysphoria can help us identify potential triggers or causes of distress. These conditions include psychological and mood disorders, including depression, anxiety, suicide/suicidal ideation, and eating disorders - as well as neurodevelopment disorders including autism.
RCCX Theory and the Highly Sensitive Immune System
I’ve spoken a lot about RCCX theory - a genetic theory that posits that approximately 20% of the population has a highly sensitive immune system, which creates a predisposition to developing a number of interconnected, overlapping health and psychiatric conditions. These conditions include the entire spectrum of psychological illness, as well as autistic features, and notably, gender dysphoria. It has been noted in the RCCX community that, as a result of RCCX genes conferring a differential hormonal milieu that alters development, many of those with presumed RCCX genes exhibit gender nonconforming behaviors and gender fluidity.
Anecdotally, it appears that those with RCCX genes are more likely to experience gender dysphoria alongside chronic and psychiatric illness. In many cases, people (and parents) have recognized that gender dysphoria is a symptom that increases with the severity of various chronic illnesses, such as Lyme disease, latent strep infections, and socioemotional disorders including autism.
The Finger Test
One interesting thing to note related to this, and one way to understand what your own hormonal milieu may have been in utero, is to look at the length of your fingers. A longer ring finger is associated with higher levels of testosterone (common in men), and a longer index finger is associated with higher levels of estrogen (common in women). If you are a woman, and your ring finger is longer than your index finger, you were likely exposed to higher amounts of androgens (testosterone) in utero and you likely have RCCX genes. If you are a man, and your index finger is longer than your ring finger, you were likely exposed to higher levels of estrogen in utero (and you also likely have RCCX genes).
Lyme Disease
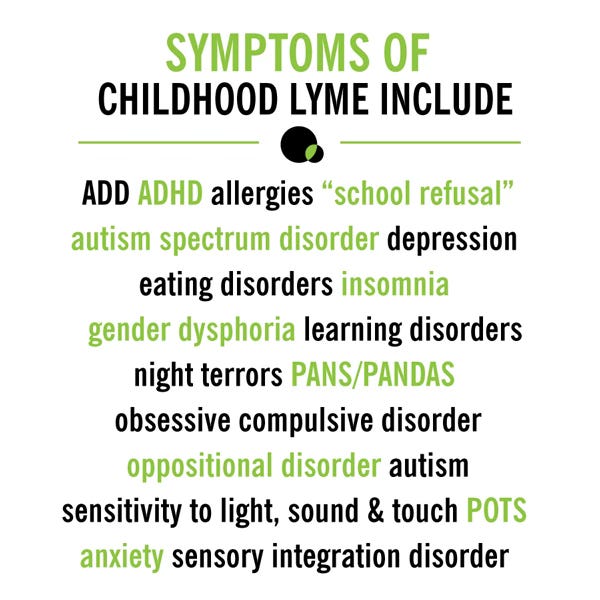
Mothers Against Lyme, an advocacy and educational group dedicated to sharing information about congenital and childhood Lyme, has identified that gender dysphoria is a symptom of childhood Lyme disease. Lyme disease is a tick-borne bacteria that can alter brain functioning and personality - but one doesn’t need a tick bite in order to contract Lyme disease as it can be passed congenitally. Which means that the onset of these symptoms may not correlate to an initial event of illness, and may simply be present and evolving from birth.
Some of the other identified psychosocial symptoms of childhood Lyme disease are presented in the graphic below.
Pediatric Acute Neuropsychiatric Disorder Associated with Streptococcus (PANDAS) & Pediatric Acute-onset Neuropsychiatric Syndrome (PANS)
Sudden onset Obsessive Compulsive Disorder (OCD) in children has been causally linked to childhood infections including strep, chickenpox, the flu, and as previously discussed, Lyme disease. Many children, parents, and specialists who treat PANDAS/PANS have noted that gender dysphoria is a common symptom of these conditions, that often resolves with treatment.
ASPIRE, the Alliance to Solve PANS & Immune-Related Encephalopathies, has identified the following set of symptoms associated with PANS and PANDAS.
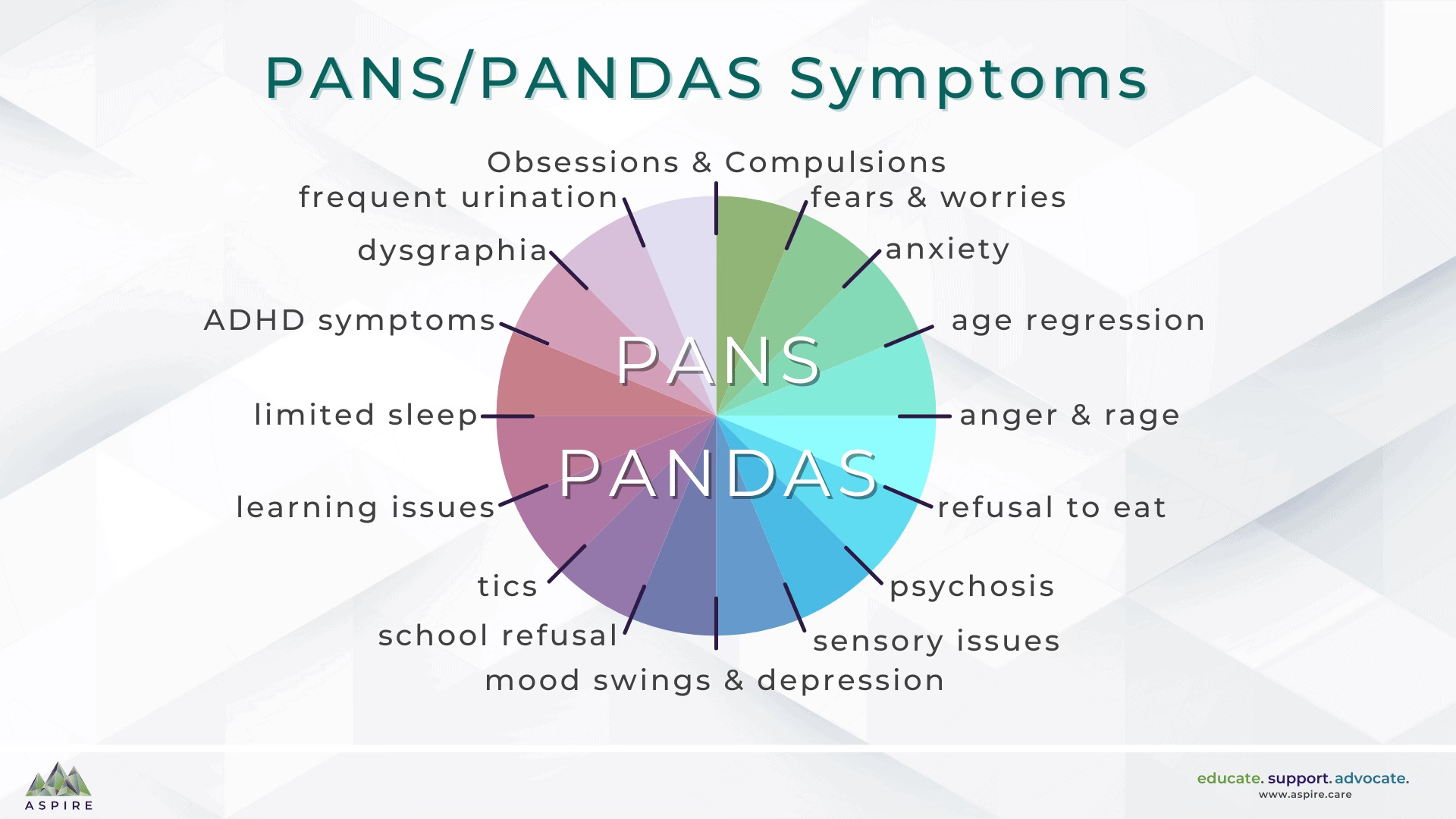
A child does not need to exhibit all of the symptoms identified above to be diagnosed with PANDAS/PANS. The PANDAS/PANS diagnostic criteria are based on the acute onset of OCD and/or eating restrictions, with concurrent symptoms in at least 2 of 7 categories of neurological, cognitive, or behavioral symptoms. Those 7 categories are:
Anxiety, Separation Anxiety
Emotional Lability and/or Depression
Irritability, Aggression, and/or Severe Oppositional Behaviors
Behavioral (Developmental) Regression
Sudden Deterioration in School Performance
Motor or Sensory Abnormalities
Somatic Signs and Symptoms, including Sleep Disturbances, Enuresis, or Urinary Frequency
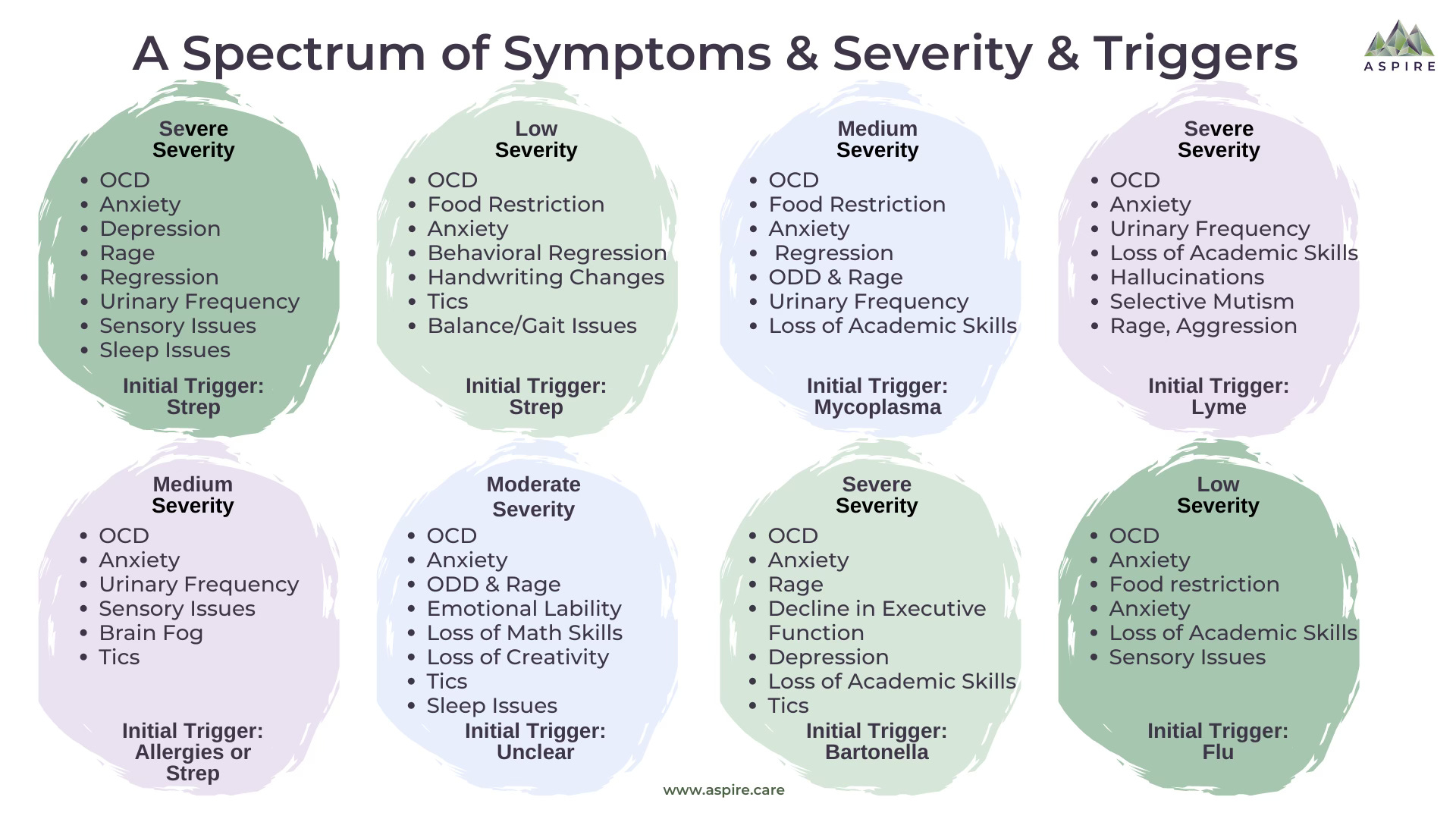
PANS/PANDAS symptom presentation, the severity of symptoms, and the trigger can vary from patient to patient. PANS/PANDAS symptoms are triggered by infections, inflammatory reactions, or metabolic disturbances.
Toxoplasmosis
Toxoplasmosis gondii is a parasite spread by cats and present in the soil, common in as much as 30-50% of the population, which can influence behavior and brain function in subtle but significant ways. While often asymptomatic in healthy individuals, chronic infection has been linked to long-term changes in neurological and hormonal pathways - and changes in personality can occur regardless of whether other symptoms associated with parasitic infection are present.
Toxoplasmosis infection has been associated with an increased risk of psychiatric disorders such as schizophrenia, as well as other neuropsychiatric symptoms including impulsivity, aggression, and altered fear response. It has also been correlated with behavioral and hormonal shifts that may influence social outcomes, such as hypemasculinization of fetuses, and increasing testosterone in women - which increases associated traits such as assertiveness, risk-taking, and dominance, and is likely why they have found that women CEOs are more likely to test positive for toxoplasmosis.
Atrazine
In 2002, a biologist and professor at UC Berkeley discovered that atrazine, an herbicide and the nation’s top selling weed-killer, is an endocrine disruptor that demasculinizes male frogs and causes them to display female characteristics - including becoming hermaphroditic. Furthermore, his research found that atrazine can cause chemical castration, and results in individuals of both sexes developing bisexual reproductive organs. He also found that atrazine is linked to reproductive cancers.
Syngenta, the company that makes atrazine, then set out to discredit both the researcher and the research. They filed a complaint against the researcher, Tyrone Hayes, with UC Berkeley, his employer, and they commissioned a psychological profile calling him a “paranoid schizo and narcissist.” They paid other scientists to discredit Hayes’ research, and lobbied the EPA to exclude Hayes’ studies.
Currently, this research is considered “controversial” simply because it is a threat to a multibillion dollar agrochemical company, and they have put a lot of money behind discrediting the findings. However, it has become more widely accepted in the 2 decades since this research first came out. Atrazine has now been found in the water supply in dozens of states, particularly in agricultural areas.
An Approach to Treatment
I personally have experienced gender dysphoria and its resolution as I treated a plethora of other chronic conditions.